
Sure, ICD-10 implementation is two years away, but there are things your medical practice should start doing today to prepare.
Coding & Documentation
Latest News
Advertisement
Advertisement
Here's a list of what your medical practice is required to provide, and what you'll get reimbursed for, regarding Medicare Annual Wellness Visits.
Here is what your medical practice needs to know about HCPCS codes, where they fit with CPT codes, and how to understand them.
The government has new tools for identifying excessive use of suspect medical codes, so you must vigilantly keep abreast of what those codes are to avoid trouble.
Coding questions? We've got the answers.
Here is how providers and coders at your medical practice can select the right E&M medical codes the first time.
You can generate over $50 per Medicare patient per year for asymptomatic screens.
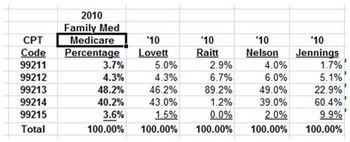
Don't let your practice be caught up in Medicare's recovery program. It's a simple matter to examine your own coding patterns and compare them to national utilization data.
Here's how to comply with all the Annual Wellness Visit requirements from CMS and avoid an audit disaster at your medical practice.
Now is the time to be sure our EHR is compliant with auditing and documentation guidelines if an audit comes your way.
The age-old tug-of-war of ways to gather and retrieve data has played a big part in where healthcare is currently with its EHR systems.
Here is an easy and quick tip that will immediately increase your inflow with minimal time and effort from treating staff at your medical practice.
It's too early for staff to learn new ICD-10 codes, but there are some other key steps your practice can take today to be ready for the looming changes.
From preparing for ICD-10 to participating in the EHR meaningful use incentive program, what’s the most difficult aspect of your daily work?
Coding questions? We've got the answers.
Want to take the pulse of your medical practice's finances? Try this easy-to-use tool to conduct a fiscal check-up on your office.
Don't miss out on easy income. Incorporating Medicare's AWV into your care plan helps both your practice and your patients.
Get coding answers on Medicare and the physical exam; combining two services; pap smear and preventive services, IV infusions and more.
Transitioning to ICD-10 presents big challenges, so turn to technology to ease your coding woes.
Physicians already have a lot on their plates, but that doesn’t mean they can overlook preparations for ICD-10. Here’s how to get them involved in the transition.
Which staff members should be on the ICD-10 documentation team, how to determine what documentation is needed, and what the key changes to anticipate are.
To ensure a successful ICD-10 transition at your medical practice, follow these seven steps from Rose Dunn of First Class Solutions, Inc
Medical coding guidance on Medicare Annual Wellness Visits; RVU reductions; physician scribes; student documentation; and more.

Juliet Santos, director of business-centered systems for HIMSS, discusses ICD-10 challenges and how technology can help a practice.
Even with a one-year delay to implement ICD-10, healthcare organizations are concerned about the magnitude of the change, and are warning providers that they still need to start preparing sooner than later.
Advertisement
Advertisement