
In many practices, partner conflict is as common as nasal infections. It may be easy to “let it go,” but that can lead to unprofessional conduct. Here’s how to diffuse disagreements and preempt disputes.
Finance
Latest News
Advertisement
Advertisement
A little price comparison can help you save big bucks on common goods and services.
Dispensing vaccines is frustrating and expensive. Here’s a shot in the arm for vaccine management.
With prices low, it may seem like a great time to buy your office space. Be wary; the advantages to ownership, while real, are balanced with disadvantages and risk. Make sure your eyes are open.
EHR companies are increasingly offering billing services, and vice versa. Is this just another way to squeeze money out of you, or does it make sense to combine the services?
Here's how to properly use E&M code 99213, including when other CPT options might be more appropriate with patients at your medical practice.
The traditional practice of primary care is complex - let’s face it, you could more accurately predict the likelihood of a patient presenting with a subdural hematoma based on his or her symptoms than you might Blue Cross’ likelihood of accepting a preauthorization for the CT scan.
Say goodbye to photocopies: Machine-readable cards could make billing and collections easier. When will payers make them widely available?
Medicare hopes to save millions with tougher billing rules and aggressive audits - changes that could cost your practice money. But if you bill right and on time, you can keep that Medicare check coming.
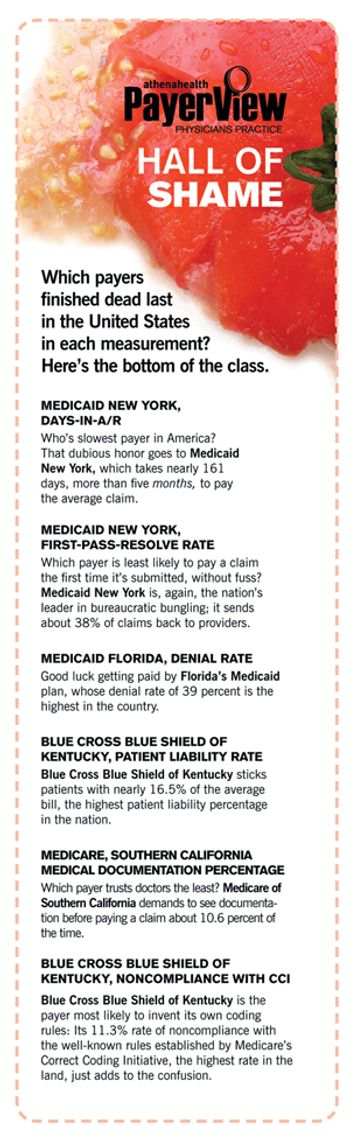
Which payers should you deal with and which should you drop? PayerView uses real claims data to rank them first to worst.
Billing “Incident-To;” Same Patient, New Problem; Moonlight Coding
Assignment of Benefits
Appeal letter for prompt payment from your medical practice payers.
Here is a sample collections letter to use at your medical practice.
Collections Letter 3
Collections Letter 3 -- Spanish
Collections Letter 2 -- Spanish
Appeal Letter Justifying Emergency Treatment
Collections Letter 1 -- Spanish
If you can't verify a patient's insurance, their signature on this form shows they know they are responsible for payment.
Appeal Letter Justifying Medical Neccessity
Assignment of Benefits -- Spanish
Use this letter when a claim is denied because a patient saw a physician in your group who is not his or her designated primary care physician.
This Advance Beneficiary Notice form, created by CMS, is best managed by the clinical team at your medical practice versus the front office staff.
Use this letter if a patient consistently refuses to pay for services rendered, and you are forced to dismiss the patient from your practice.
Advertisement
Advertisement
Trending on Physicians Practice
1
8 charges your practice is probably never billing
2
8 jobs in your practice only one person knows how to do
3
Most practices cut the wrong thing first, with Shawntea Gordon of Atlas & Perpetua Healthcare Consulting
4
Team building to enhance staff morale
5